|
MAPS, in conjunction with California NORML, has been working since 1993 to sponsor scientific research into the effects of vaporizers and waterpipes in filtering the constituents of inhaled marijuana. Our goal was to determine if waterpipes or vaporizers could reduce the health risks of smoking marijuana. From 1993 to 2002, we sponsored research at DEA-licensed laboratories testing the content of combusted and vaporized marijuana for cannabinoid, particulate and carbon monoxide levels (see MAPS Bulletin articles from XXXX year, XXXY year, XXXZ year, etc). 1993:
http://www.maps.org/news-letters/v04n3/04310pip.html In a prolonged triumph of Drug War politics over science, our vaporizer research has been blocked since June 2003 by the National Institute on Drug Abuse (NIDA), which has a monopoly on the supply of marijuana that can be used in research. For more than five and a half years, NIDA has rejected and/or ignored our repeated requests (including one lawsuit for “unreasonable delay”) seeking to purchase 10 grams of marijuana to continue our studies. NIDA uses its monopoly to obstruct studies into both the beneficial medical uses of marijuana as well as into drug delivery devices that might increase the chances of FDA-approval of marijuana as a prescription medicine, and might decrease harms associated with the non-medical uses of marijuana. Most recently, Gregory Goldstein, HHS Senior Public Health Advisor, Office of the Assistant Secretary of Health, sent a letter to Chemic on January 23, 2009, saying that HHS would require a validation study showing that Chemic could reliably measure various cannabinoids before it would even review Chemic's November 6, 2008 reply to the June 18, 2008 PHS/NIDA critique of Chemic's January 16, 2008 protocol. In our initial studies, when NIDA wasn’t so politicized about medical marijuana, we learned early on that waterpipes don't help filter out undesirable particulate matter, although waterpipes may help reduce certain water-soluble gases. In contrast, vaporizers do eliminate combustion products and address the Institute of Medicine's 1999 recommendation for the development of non-smoking delivery systems for the medicinal use of marijuana. Vaporizers are the only non-smoking delivery system that use the marijuana plant itself, rather than patented and for-profit pharmaceutical company marketed marijuana extracts in spray, lozenge, drops, or pill form. In contrast, vaporizers could conceivably be used in conjunction with material that patients grow themselves or obtain in other ways, at substantially reduced cost as compared to patented products, and, as our preliminary research suggests, at virtually no increased health risk or reduced efficacy. While the use of vaporizers in medical marijuana research is the most politically desirable route, since they don't involve smoking, we plan to include groups that smoke as well as vaporize marijuana in future clinical studies. We would be surprised if there are significant differences in safety and efficacy for most patients, due to the lack of evidence linking marijuana smoking and cancer and the increasing body of evidence about the anti-tumor properties of marijuana. MAPS’ Two Prerequisites For FDA Drug Development Research Unlike NIDA, MAPS and CaNORML believe that the medical use of marijuana is an issue that needs to be resolved scientifically rather than politically. MAPS has identified two essential prerequisites before we can justify starting a serious ($10 million) drug development effort conducting studies under FDA’s Investigational New Drug (IND) program. The first prerequisite is that a vaporizer device needed to be accepted by FDA for use in clinical research. This objective has been met, since our initial vaporization research was used by Dr. Donald Abrams to obtain a $137,000 grant in 2004 from California's Center for Medicinal Cannabis Research (CMCR) for a Phase I vaporizer research protocol. The study compared subjective effects, cannabinoid blood levels and carbon monoxide levels in exhaled breath and used the Volcano vaporizer. The study concluded that vaporization produced similar cannabinoid blood levels and subjective effects as smoking but with reduced carbon monoxide. MAPS second prerequisite is obtaining DEA permission for our own independent supply of marijuana, thereby breaking the NIDA monopoly so we can work directly with FDA without the obstruction, delays and outright refusal of NIDA to provide the necessary marijuana. We’ve been working since 2001 with Prof. Lyle Craker, UMass Amherst, seeking a DEA license for a MAPS-sponsored medical marijuana production facility. On February 12, 2007, Prof. Craker won a DEA Administrative Law Judge (ALJ) hearing when DEA ALJ Mary Ellen Bittner found that it would be in the public interest for DEA to issue a license to Prof. Craker and recommended that DEA issue Prof. Craker a license, thereby ending the federal monopoly on supply. DEA has not yet issued its required final ruling, following its highly successful strategy of delay which has prevented marijuana from becoming an FDA-approved prescription medicine for almost 40 years, since 1970 when the use of marijuana to control nausea associated with cancer chemotherapy was reported. MAPS is working with the Americans for Safe Access and other drug policy reform organizations seeking to persuade the Obama Administration to issue Prof. Craker his license. For further background, also see:
Project status: April 1, 2004. Congressman Mark Souder, Chairman of the U.S. House Government Reform Subcommittee on Criminal Justice, Drug Policy, and Human Resources, held a hearing about "Marijuana and Medicine: The Need for a Science-Based Approach." MPP Executive Director Rob Kampia testified (video and transcript) and answered questions (video and transcript). During his comments, he discussed the importance of MAPS' vaporizer research efforts as well as the UMass Amherst project. March 19, 2004. Dr. Donald Abrams receives word that his FDA-approved Phase I vaporizer study is now ready to enroll subjects. He will be comparing cannabinoid and carbon monoxide levels and subjective effects in subjects who at different times inhale either marijuana smoke from a burning cigarette or marijuana vapors from the Volcano vaporizer. Being able to use a vaporizer in FDA-approved clinical trials is one of MAPS' two prerequisites to justifying the expense of a $5 million effort to develop marijuana into an FDA-approved prescription medicine, the other prerequisite being an independent source of supply of marijuana for research other than using material from the National Institute on Drug Abuse (NIDA). March 17, 2004. In an effort to find out what is going on with the Health and Human Services (HHS) review of the scientific merit of the vaporizer protocol, an exchange of email took place today between Willem Scholten, Head of the Dutch Office of Medicinal Cannabis and Rear Admiral, Assistant Surgeon General and Deputy Assistant Secretary for Health (Operations) Arthur J. Lawrence. Willem Scholten inquired about the status of the review. Dr. Lawrence replied that the responsibility for the review was being shifted from his office and at the moment he didn't know exactly to where or what was going on. He was, however, sure that, " this protocol will, as all proposed protocols for this sort of research are, be given fullest consideration and deliberation in the scientific review." Somewhat dissatisfied with the review seemingly being on the slow track to nowhere, MAPS President Rick Doblin replied to Dr. Lawrence. He requested whatever help Dr. Lawrence could offer in expediting the review, noting that the protocol was first submitted for review on June 24, 2003 and that all we were asking for was to purchase 10 grams of NIDA marijuana and import 10 grams from the Dutch. He concluded by stating, "The vaporizer research project is part of MAPS' efforts to work through the rigorous FDA drug review process to conduct exactly the sort of studies that DEA, ONDCP, NIDA, IOM, all claim to want to see conducted. Given the difficulties in purchasing a tiny amount of marijuana for this simple vaporizer research protocol, it should not be surprising why so many States have gone ahead and legalized the medical use of marijuana in one form or another without waiting for the FDA to approve its medical use on the basis of double-blind, randomized, placebo-controlled research." Also, Dr. Scholten informed MAPS that some vaporizer research with the same Volcano device was being conducted in the Netherlands. We've sent a message to the researcher and look forward to collaborating and sharing information. January 29, 2004. The scientific review of the vaporizer protocol being conduced by the federal Dept. of Health and Human Services is now being supervised by Assistant Surgeon General Arthur J. Lawrence Ph.D. Mr. Joel Egertson, senior drug policy advisor to the Secretary of HHS, has retired and the responsibility for the review has been reassigned. A revised and updated package of information has been submitted today by Chemic Labs to Assistant Surgeon General Lawrence. If HHS determines that the vaporizer protocol is scientifically meritorious, NIDA will agree to sell us 10 grams of marijuana and DEA will be required to address our request to import 10 grams of marijuana from the Dutch Office of Medicinal Cannabis. The protocol is a rigorous investigation and, if reviewed in an unbiased manner, will be determined to be scientifically meritorious. MAPS initially requested permission in June 2003 to purchase marijuana from NIDA and import marijuana from the Dutch. This delay is clear evidence why NIDA's monopoly on supply of research marijuana serves more to obstruct than to facilitate marijuana research. December 16, 2003. MAPS received a grant of $13,000 for further vaporizer research from the Marijuana Policy Project. The grant includes $5,000 for the writing of a scientific paper about the results of the research for submission to a journal indexed in Medline. Also included is $8,000 for a study of the cannabinoid content of each of the 1st, 2nd, and 3rd balloons created by the Volcano vaporizer from the same sample of marijuana. We want to see if we can eliminate the use of the 3rd balloon in clinical research if only minimal amounts of cannabinoids are released the third time the same sample is heated and vaporized. This study can be conducted only after we have been able to obtain approval from HHS to purchase 10 grams of marijuana from NIDA, a time-consuming hurdle that wouldn't be necessary if MAPS had its own independent source of supply of marijuana that could be used in federally-approved research (as we have with MDMA and psilocybin, for example). December 4, 2003. The manufacturers of the Volcano vaporizer that MAPS and CaNORML are using in our vaporizer research, STORZ & BICKEL GMBH & CO. KG, announce that they have received the Dr. Rudolf Eberle Prize, the prize for innovation of the State of Baden-Wurttemberg. This prize has been awarded on an annual basis since 1985 to small and medium-sized industrial and craft firms who have successfully implemented outstanding technical innovations. The prize committee uses the criteria of technical progress, special entrepreneurial achievement and the economic success of the innovation to make its decision. November 14, 2003. Vaporizer protocol likely to start early in 2004. According to Dr. Donald Abrams, "As far as I know we are awaiting our award from CMCR. All approvals are granted and we plan to commence the vaporizer protocol in January 2004." October 10, 2003. The analytical lab conducting the vaporizer research has received replies from NIDA and the DEA regarding its requests to import 10 grams of marijuana from the Dutch Office of Medicinal Cannabis and to purchase 10 grams from the National Institute on Drug Abuse (see entry below for June 24, 2003). The reply from NIDA came from Joel Egertson, Senior Drug Policy Advisor to the Secretary of Health and Human Services (HHS). Mr. Egertson wrote, "It has been determined that there is insufficient information in the application to judge the merits of the proposal. " Mr. Egerston had been submitted the protocol for which the 10 grams was requested but asked for additional information that has already been generated from previous research protocols and has already been submitted to the FDA. This additional information will be submitted to Mr. Egerston very soon for HHS review. The reply from DEA indicated that it would not proceed with the import permit until the scientific merits of the protocol had been accepted by HHS. While a decision on these requests has been delayed, we believe we can adequately address all the issues raised by HHS and DEA. Yet again, this prolonged process to purchase tiny quantities of marijuana for important privately-funded research demonstrates the need for MAPS to sponsor a privately-funded facility to produce marijuana for federally-approved research, as we are attempted to do in partnership with Prof. Craker at UMass Amherst. June 24, 2003. Grant for Vaporizer Study with Humans Approved Contingent upon Regulatory Approval. California's Center for Medicinal Cannabis Research (CMCR) preliminarily approved Dr. Donald Abrams' Phase I vaporizer research protocol and grant application, amounting to slightly more than $137,000, contingent upon the protocol obtaining all the necessary regulatory approvals. The study will compare subjective effects, cannabinoid blood levels and carbon monoxide levels in exhaled breath in subjects on six different days, three days smoking 400 mgs of marijuana of either 1.7 % THC, 3.5% THC or 7% THC, and three days vaporizing 400 mgs of marijuana of either 1.7 % THC, 3.5% THC or 7% THC. The protocol now goes to FDA for its review, finally. The big question is whether the FDA will want more data than MAPS and California NORML have already gathered on the Volcano (www.vapormed.de) or will accept the data we have already submitted, which is more than FDA has about what is in marijuana smoke post-combustion. We should hear from FDA within 4-6 weeks or so. Also reviewing the protocol will be NIDA (since NIDA pot is being requested), DEA (supposedly to see what it can do to prevent the diversion of research supplies), and the Research Advisory Panel of California (which reviews all Schedule I research in California). The key review will be by FDA, since it will decide whether or not MAPS and California NORML need to raise more funds for additional vaporizer research. June 24, 2003. Maps Working to Import Dutch Cannabis for Research. MAPS has completed negotiations with the head of the Dutch Office of Medicinal Cannabis for the importation of ten grams of high THC, high CBD marijuana for use in the next phase of the vaporizer research project. Chemic Laboratories, where the project will be conducted, has submitted an application to the DEA for an import license. This request to the DEA is, to our knowledge, the first attempt to import the marijuana plant from the Netherlands, through the newly established Office of Medicinal Cannabis. Chemic Laboratories has also submitted a request to NIDA for ten grams of its best quality product for the vaporizer project. California NORML/ MAPS Press Release — May 2, 2003
 Dale Gieringer, Ph.D. (canorml@igc.apc.org) MAPS Bulletin, Spring 2003; Volume XIII, Number 1 April 15, 2003. Vaporizer Study Report. The Vaporizer report is now available. The findings show substantial reduction (about 99%) in certain toxins in the vapor as compared to marijuana smoke, and substantial amounts of cannabinoids produced by the vaporizer. The results could hardly have been better. This report has been submitted to FDA as part of Dr. Donald Abrams' IND application to study subjective effects and cannabinoid blood levels in subjects who both smoke marijuana and then at a later time inhale marijuana vapors. We should hear from FDA in early May about what additional information, if any, it needs to have before deciding if the vaporizer can be used in a clinical trial. January 21, 2003. MAPS and CANorml sign a contract for a $25,000 protocol study to evaluate the contents of the vapor stream from the Volcano Vaporizer (http://www.vapormed.de). The purpose of the study is stated in the contract as follows: This protocol is intended to provide guidance on the completion of an extraction evaluation of emissions produced when marijuana is vaporized using the Volcano; to provide evidence of product efficiency to MAPS, which would subsequently design and seek agency (FDA) approval for the protocol development and initiation of a Phase I clinical investigation comparing cannabinoid blood levels in subjects smoking (i.e. pyrolysis) marijuana versus marijuana vaporized with the Volcano, and to meet the requirements of cGMP: 21 CFR Part 160. We expect the study to be completed by the end of March 2003. Here are urls for various vaporizers: Dale Gieringer, Ph.D. NORML California State Coordinator (canorml@igc.apc.org) MAPS Bulletin, Spring 2001. Volume XI, Number 2. Medical marijuana patients may be able to protect themselves from harmful toxins in marijuana smoke by inhaling their medicine using an electric vaporizer, according to initial results of a study by the Multidisciplinary Association for Psychedelic Studies (MAPS) and California NORML. Research expenditures to date are roughly $50,000. The study showed that it is possible to vaporize medically active tetrahydrocannabinol (THC) by heating marijuana to a temperature short of the point of combustion, thereby eliminating or substantially reducing potentially harmful smoke toxins that are normally present in marijuana smoke. Vaporizers may therefore substantially reduce what is widely regarded as the leading health concern associated with marijuana, namely respiratory harm due to smoking. In addition, many medical marijuana patients say they prefer vaporizers because they deliver smoother, less irritating medication. MAPS and NORML sponsored the study in the hopes of helping medical marijuana patients and others reduce the health risks of smoking marijuana. A major obstacle to approval of natural cannabis by the Institute of Medicine (IOM) in its 1999 report, "Marijuana and Medicine," was that smoking is an "unhealthy" delivery method. The IOM report failed to note the possibility of vaporization. The MAPS-NORML study tested a device called the M1 Volatizer(R), an aromatherapy vaporizer developed by Alternative Delivery Systems, Inc. It consisted of an electric heating element in a chamber that radiates heat downwards over a sample of marijuana contained in a standard bowl. Output from the vaporizer was analyzed and compared to smoke produced by burning the sample. The vaporizer produced THC at a temperature of 200° C. (392° F.) while completely eliminating three measured toxins - benzene, a known carcinogen, plus toluene and naphthalene. Temperatures of around 200° C. appear to be most efficient for vaporization. The potency of the cannabis in the study was on the order of 10% - 12%. Significant amounts of THC (around 5%-6%) begin to be released at 180° C., with slightly more (7% or 8%) at 200° C. Carbon monoxide and smoke tars were both qualitatively reduced by the vaporizer, but additional testing is needed to quantify the extent of the decrease. The vaporizer study was undertaken as a follow-up to a previous MAPS-NORML marijuana smoking device study, which concluded that vaporizers offered the best prospects for smoke harm reduction: http://maps.org/news-letters/v06n3/06359mj1.html MAPS and NORML are currently seeking support for further research and development of vaporizers. Research is presently underway to explore the optimal temperature and conditions for vaporization. An additional $85,000 is needed to provide accurate measurement of carbon monoxide and other toxins, such as polycyclic aromatic hydrocarbons. Further studies may be needed to explore alternative device designs and the effects of different consistencies, potencies and preparation methods of the samples of marijuana.
Dale Gieringer, Ph.D. (canorml@igc.apc.org MAPS Bulletin, Summer 1996. Volume VI, Number 3. September 21, 2000 update: MAPS and CA-NORML are sponsoring a new vaporizer study. Testing and data analysis have been completed. A detailed report will be issued soon. The design and cost of additional studies are currently being discussed with the analytical lab. The new study is a $25,000 proof of principle study designed to determine if marijuana vaporizers can indeed reduce particulate matter and carbon monoxide as compared to the combustion of marijuana. We have a very high-tech lab doing the research, but unfortunately the lab wants to remain anonymous. They are concerned about becoming known as a place with marijuana (all they have is 5 grams!), but the major reason for their reluctance to get publicity is due to industrial espionage. They do lots of work for major pharmaceutical companies who want discretion, so they don't advertise. I was personally recommended to them by an organic chemistry company that is making psilocybin for MAPS for a U. of Arizona study of psilocybin in the treatment of OCD. Anyway, the results of the vaporizer study do show substantial reductions in particulate matter and in carbon monoxide. I conceive of this study as contributing to the argument in favor of permitting patients to grow and use their own marijuana, instead of having to purchase patented, FDA-approved cannabinoid or marijuana-extract products from Unimed or GW Pharmaceuticals. Vaporizers are the only non-smoking marijuana delivery systems that can be used with home-grown marijuana. We are trying to create evidence to show that there is a favorable risk/benefit ratio from using high-potency marijuana in vaporizers. The main tradeoffs that patients will face are slightly highly but probably not clinically significant health risks but lower price from high-potency marijuana delivered in vaporizers as compared to Unimed or GW products. Efficacy will probably be similar. The health effect of wealth (the impact on the health of patients from the extra money they save from using home-grown in vaporizers as compared to other products) will, perhaps, outweigh the additional health risks. This is all speculative and there is certainly a major need for FDA-approved products that can be paid for by insurance, since home-grown used with vaporizers will probably not become approved by FDA anytime soon, at least not in the current political climate.
See also:
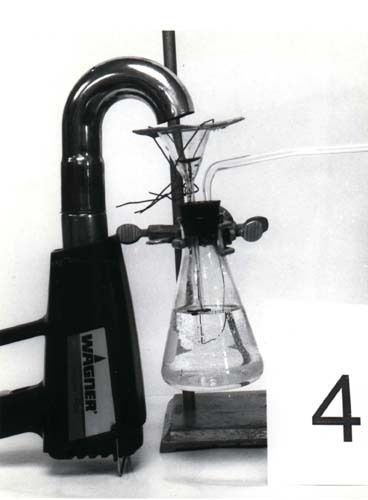
Seven Devices Tested The study, which was supported by the Drug Policy Foundation and private donors, was conducted at a research lab with expertise in the analysis of various chemical properties of tobacco and marijuana. Researchers tested the smoke from seven different sources: a regular rolled joint, a joint with a cigarette filter, three different waterpipes, and two vaporizers, designed to heat marijuana to a temperature where psychoactive vapors form without producing smoke. The waterpipes included a standard bong (Picture #1), a small portable device with a folding pipestem (Picture #6), and a battery-operated model with a motorized paddle to thoroughly mix the smoke in the water (Picture #3). The first vaporizer (Picture #5), commercially produced in Canada, consisted of a battery-powered metal hot plate inside a jar to trap the marijuana vapor. The second (Picture #4) was a homemade, hybrid apparatus, in which vapors were produced by a hot air gun and then drawn through a beaker of water, thereby combining vaporization with water filtration. The smoke was produced from standard NIDA-supplied marijuana drawn through a smoking machine adjusted to mimic the puff length of marijuana smokers. Focus: Cannabinoid/Tar Ratio The study focused on two key components of the smoke: (1) total solid particulates, or tars, which are noxious waste by-products of burning leaf like those from tobacco; and (2) cannabinoids, the chemicals distinctive to marijuana, including its major psychoactive ingredient, delta-9-tetrahydrocannabinol (THC), and its two commonest chemical relatives, cannabinol (CBN) and cannabidiol (CBD), which are only weakly psychoactive but may have medical benefits. Like tobacco, marijuana tars are rich in carcinogenic compounds known as polycyclic aromatic hydrocarbons, which are a prime culprit in smoking-related cancers. However, cannabinoids themselves are not carcinogenic. An obvious way to protect smokers' health is therefore to minimize the content of smoke tars relative to cannabinoids. One way to do this is to increase the THC potency of the marijuana. Assuming smokers adjust their smoke intake to the cannabinoid dosage, the higher the concentration of cannabinoids, the lower the amount of tars they are likely to consume.
Joints and Waterpipes Surprisingly, the unfiltered joint outperformed all devices except the vaporizers, with a ratio of about 1 part cannabinoids to 13 parts tar. This disturbingly poor ratio may be explained by the low potency of the NIDA-supplied marijuana used in the study, which was around 2.3%.
Vaporizers The vaporizer results appeared more promising, but confusing. The two vaporizers were the only devices to outscore unfiltered joints in terms of raw cannabinoid/tar ratio. The electric hotplate vaporizer did best, with a performance ratio about 25% higher than the unfiltered joint. The hot air gun was just marginally superior, but might have done better had it not been for its water filtration component.
The results clearly indicate that more developmental work needs to be done on vaporizers. Theoretically, an ideal vaporizer could minimize production of tars by holding the temperature above the point at which THC vaporizes, but below that where carcinogenic hydrocarbons are produced by combustion [Note] In practice, both vaporizers produced over ten times more tars than cannabinoids, indicating that there is plenty of room for improvement. In the late 1970s, a vaporizer known as the Tilt appeared on the market. According to the manufacturer, laboratory tests showed that it released 80% more THC and 79% less tar than a regular pipe, a performance ratio almost ten times better than any observed in this study. It is to be hoped that these impressive results can be replicated in the future. Unfortunately, the Tilt was withdrawn from the market in the early 1980s due to the passage of anti-paraphernalia laws. As for waterpipes, the prospects for improvement appear more dubious. It has been suggested that the performance of waterpipes could be improved by using liquids other than water or by changing the temperature of the liquid. However, it seems doubtful whether such tactics would circumvent the basic problem of separating the tars from the sticky cannabinoids. Are Waterpipes Counterproductive? The study results are obviously discomforting to waterpipe enthusiasts, many of whom prefer the cooler, milder smoke they produce, and have naturally assumed it is also more healthful. Unfortunately, however, the study indicates that waterpipes may actually be counterproductive in increasing consumption of carcinogenic tars. Nonetheless, it is still premature to judge that waterpipes are actually unhealthful, since they may filter out other, non-solid smoke toxins occurring in the gas phase of the smoke, which was not analyzed in the study. Noxious gases known to occur in marijuana smoke include hydrogen cyanide, which incapacitates the lung's defensive cilia; volatile phenols, which contribute to the harshness of the taste; aldehydes, which promote cancer; and carbon monoxide, a known risk factor in heart disease. Previous studies indicate that water filtration may be quite effective in absorbing some of these [Nicholas Cozzi, Effects of Water Filtration on Marijuana Smoke: A Literature Review, MAPS Newsletter, Vol. IV #2, 1993]. If so, waterpipes might still turn out to have net health benefits. MAPS and California NORML are planning to undertake a second phase of the waterpipe study for the purpose of analyzing the gaseous phase of marijuana smoke. In the meantime, the easiest way for most smokers to avoid harmful smoke toxins may be simply to smoke stronger marijuana. This strategy is apt to be more effective than any smoke filtration device. By simply replacing the low, 2.3% potency NIDA marijuana used in this study with high-quality 12%-sinsemilla, smokers could presumably reduce their tar intake by a factor of five while still achieving the same effect. Further improvements could be had by using pure THC or hash oil, which has been tested at potencies of 60%. The notion that high-potency marijuana is less harmful directly contradicts official government propaganda, which maintains that marijuana has become more dangerous since the '60s due to increased potency. This claim appears to rest less on scientific evidence than on the desire to frighten the public. A careful analysis of government data by Dr. John Morgan has shown that the supposed increase in potency has been greatly exaggerated [American Marijuana Potency: Data Versus Conventional Wisdom, NORML Reports (1994)]. In any case, however, there is no good reason to presume that higher potency marijuana is more harmful, given the potential respiratory benefits of reduced smoke consumption. The hazards of excessive potency are purported to be an increased risk of acute overdose and greater susceptibility to dependency. However, both problems can be avoided if users adjust their dosage to potency. For most users, such hazards may well be outweighed by the benefits of reduced smoke consumption. Research in Australia The Australian government is currently conducting another study that may cast further light on the effects of potency variations. The study is designed to determine baseline THC, tar, and carbon monoxide levels from marijuana and marijuana-tobacco mixtures smoked through joints and waterpipes. The samples being tested come from police seizures in six different Australian states. Researchers say that they have observed "incredible" variations in tar and THC potency among different samples. Their report is expected shortly. THC Transfer Rate The MAPS-NORML study provides new information on the efficiency of different devices in delivering THC from marijuana to the user. Previous studies have shown that 60% - 80% of the THC burned in joints or waterpipes is lost in slipstream smoke, adhesion to the pipestem and bowl, pyrolysis, etc. [Mario Perez-Reyes, Marijuana Smoking: Factors that Influence the Bioavailability of Tetrahydrocannabinol, in C. Nora Chiang and Richard Hawks, ed., Research Findings on Smoking of Abused Substances, NIDA Research Monograph 99, 1990]. The percentage of total THC delivered to the user is called the THC transfer rate. The unfiltered joint scored surprisingly well in smoking efficiency, coming in second place with a transfer rate close to 20%. The portable waterpipe did slightly better, and the bong slightly worse. The other devices did notably worse. The vaporizers and electric waterpipe did especially poorly, with transfer rates less than one-third that of the top three devices. Thus, heavy smokers could literally be blowing most of their stash away with bad pipes.
Note:
California NORML |


 Another strategy is to try to reduce the tars in the smoke with some kind
of filtering device. Obviously, this is beneficial only to the extent that
THC isn't also reduced, thereby inducing users to smoke more to
compensate. A major aim of the study was to determine the efficacy of
various smoking devices at reducing the concentration of tars relative to
cannabinoids. The performance of each device was accordingly rated in
terms of the cannabinoid-to-tar ratio in its smokestream.
Another strategy is to try to reduce the tars in the smoke with some kind
of filtering device. Obviously, this is beneficial only to the extent that
THC isn't also reduced, thereby inducing users to smoke more to
compensate. A major aim of the study was to determine the efficacy of
various smoking devices at reducing the concentration of tars relative to
cannabinoids. The performance of each device was accordingly rated in
terms of the cannabinoid-to-tar ratio in its smokestream.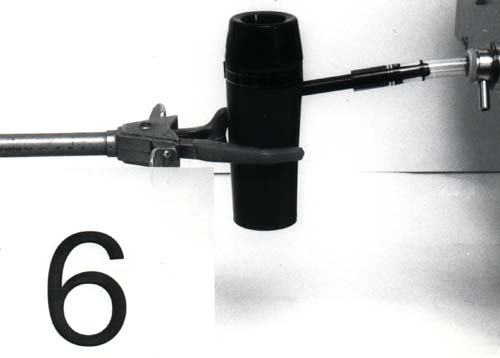 Disappointingly, waterpipes performed uniformly worse than the unfiltered
joint. The least bad waterpipe, the bong, produced 30% more tar per
cannabinoids than the unfiltered joint. Ironically, the pipe with the
electric mixer scored by far the worst of any device. This suggests that
water filtration is actually counterproductive, apparently because water
tends to absorb THC more readily than noxious tars. Like the waterpipes,
the cigarette filter also performed worse than the unfiltered joint, by
about 30%. Researchers speculate this is because cannabinoids are
exceptionally sticky and adhere to other solids. Hence, any filtration
system that picks up particulates is likely also to screen out
cannabinoids.
Disappointingly, waterpipes performed uniformly worse than the unfiltered
joint. The least bad waterpipe, the bong, produced 30% more tar per
cannabinoids than the unfiltered joint. Ironically, the pipe with the
electric mixer scored by far the worst of any device. This suggests that
water filtration is actually counterproductive, apparently because water
tends to absorb THC more readily than noxious tars. Like the waterpipes,
the cigarette filter also performed worse than the unfiltered joint, by
about 30%. Researchers speculate this is because cannabinoids are
exceptionally sticky and adhere to other solids. Hence, any filtration
system that picks up particulates is likely also to screen out
cannabinoids.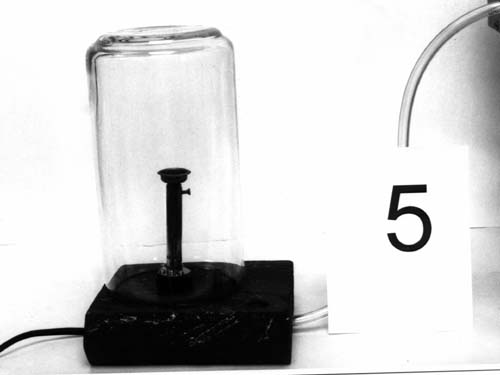 However, the situation was complicated by the fact that the cannabinoids
produced by the electric hotplate vaporizer were unusually high in CBN,
leaving 30% less THC as a percentage of the total cannabinoids than with
the other smoking devices. Since CBN is not psychoactive like THC,
recreational users might be expected to consume more smoke to make up for
the deficit. (The situation may be different for medical users, who could
experience other, medicinal benefits from CBN). For this reason, it seemed
advisable to recompute the performance efficiencies of the vaporizers in
terms of THC, rather than all cannabinoids. When this was done, the
However, the situation was complicated by the fact that the cannabinoids
produced by the electric hotplate vaporizer were unusually high in CBN,
leaving 30% less THC as a percentage of the total cannabinoids than with
the other smoking devices. Since CBN is not psychoactive like THC,
recreational users might be expected to consume more smoke to make up for
the deficit. (The situation may be different for medical users, who could
experience other, medicinal benefits from CBN). For this reason, it seemed
advisable to recompute the performance efficiencies of the vaporizers in
terms of THC, rather than all cannabinoids. When this was done, the
 The reason for the excess CBN from the hotplate vaporizer remains
unexplained. Because CBN is produced from THC by chemical oxidation, it
has been suggested that the device somehow exposed the sample to too much
oxygen. However, there is no evidence that this was the case. As for the
second, hybrid vaporizer, it seems likely that its performance could have
been improved by deleting its water component.
The reason for the excess CBN from the hotplate vaporizer remains
unexplained. Because CBN is produced from THC by chemical oxidation, it
has been suggested that the device somehow exposed the sample to too much
oxygen. However, there is no evidence that this was the case. As for the
second, hybrid vaporizer, it seems likely that its performance could have
been improved by deleting its water component.
{kind=link}
{kind=link}